
This is the first Plain Speaker report on the hospital cuts plans that are scheduled for public consultation, starting at the end of February.
In it you can find out about:
- Key elements of the plan – called Right Care Right Time Right Place
- Why we need the NHS Reinstatement Bill
- Why we need to keep both A&Es open
- Lack of evidence that the proposals will deliver health care to the required standards
- How successive governments have prioritised bailing out the bankers above properly funding public services for their own people
- How Monitor (the NHS “market competition” regulator) and management consultancy company Ernst and Young (with a vested interest in NHS privatisation) are behind the CCGs’ proposal
- A pattern of sacrificing publicly owned hospitals to protect PFI bankers’ profits
Hospital cuts schemes like this are being rolled out all across the country, under various names. But they are all working to the same plans.
The only real solution to the problems that the Clinical Commissioning Groups hope to solve through their hospital cuts proposals is to restore the NHS to a fully publicly owned, run and funded health service, that it is the duty of the Secretary of State to provide, and that restores its founding principles of universality, comprehensiveness and being free at the point of need. Please ask your MP to vote for the cross-party NHS Reinstatement Bill in the House of Commons on 11 March.
The “Right Care Right Time Right Place” Pre-Consultation Business Case could just as well be called “Less Care, Whenever and Wherever You Can Find It”
Its proposals will be equally bad for the people of Calderdale and for Huddersfield people.
The basic plan is to
- Knock down Huddersfield Royal Infirmary (HRI) and sell off the site for development.
- Build a 119 bed planned care clinic plus outpatients and and urgent care centre on Acre Mill across the road from HRI.
- Take services out of the hospital and put them in the “community” (so-called Care Closer to Home).
- Expand Calderdale Royal Hospital (CRH) from 400-ish beds to 615 and make it the unplanned (acute) care hospital and emergency care centre for both Kirklees and Calderdale, plus an urgent care centre. (The urgent care centres will treat patients for minor illnesses and accidents.)
- Set up an urgent care centre in Todmorden.
- Take more A&E patients to CRH as a result of the closure of Dewsbury A&E and its replacement with an urgent care centre

Wrath and anxiety has erupted in Kirklees at the news that Huddersfield would lose its A&E if these plans are carried out – while people in Calderdale are wearily still plodding along as we have been for the last two years, campaigning to keep both A&Es open, with help from Huddersfield Keep Our NHS Public.
Why we need to keep both A&Es open
The main thing as far as I can see from reading the Pre Consultation Business Case is that if these proposals were to happen, they would be equally bad for people in Calderdale and people in Huddersfield.
This is why Save CRH facebook group, Calderdale & Kirklees 999 Call for the NHS, Calderdale 38 Degrees NHS Campaign, Huddersfield Keep Our NHS Public, Calderdale Green Party and Kirklees Green Party are all campaigning to keep both A&Es open 24/7 – and have been for the last 2 years since the proposals were first made public.
(These are just the groups currently known to Plain Speaker – if there are more, please add them in the comments box at the end of this post.)
Obviously, the CCGs’ stated intention is not to provide less and poorer quality healthcare -the PCBC says (p214):
“The whole population of Calderdale and Huddersfield should benefit from the proposal.”
But when a nearby A&E closes, the inpatient death rate in hospitals that still have an A&E goes up, as a big 2014 Californian study has shown. Patients who still had a local A&E department had 5 percent higher odds of inpatient mortality than admissions not occurring near a closure. This was because of overcrowding from a neighbouring area where the A&E had closed. How is that going to be good for people in Calderdale?
And when an A&E closes, the people who used to use that A&E have to travel further to reach A&E. This too increases the death rate – there is a clear association between increased distance to A&E and increased death rate.
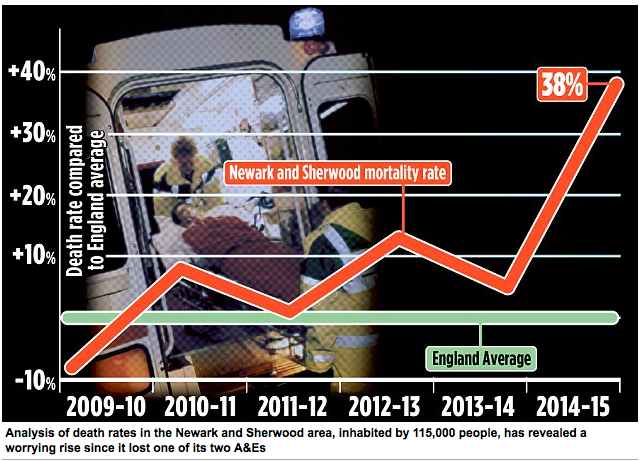
After Newark Hospital A&E closed, Say Yes to Newark Hospital campaign group obtained data through a Freedom of Information request that showed increased mortality rates for emergency patients from Newark who had to travel to A&E, but death rates had fallen for other patients visiting the same hospitals who had less distance to travel. Based on these figures, a Mail on Sunday report claimed death rates for emergency patients
from Newark had shot up 37% since the closure of their A & E.
And two academic studies – reported in the Journal of Emergency Medicine and the Journal of Trauma and Acute Care Surgery – have also found that that increased distance to A&E is associated with increased risk of death.
That will definitely not be good for people in Huddersfield.
And that’s nowhere near the half of it.
No evidence that the proposals will deliver health care to the required standards
There is the small problem that the Clinical Senate (a group of doctors) says the hospital services proposals are so unclear that they can’t:
“answer questions regarding the ability of this model to deliver the standards proposed.”
The Clinical Senate is equally dubious about the community care/Care closer to home care model, which aims to move services out of the hospitals. It also says this model is not clear enough to be able to tell if it will “deliver to the standards proposed.”
So it isn’t just from notions of solidarity that we need to demand both A&Es stay open 24/7, – but because there are no winners in this misguided plan, for the people of Calderdale or the people of Huddersfield.

Some Huddersfield folk are blaming this on Calderdale Royal Hospital for its PFI debt, and on Greater Huddersfield CCG for selling out Huddersfield people by voting to take the plan to public consultation.
But who or what is really behind this plan?
Successive governments would rather bail out the bankers, rather than properly fund public services for their own people
After the bankers wrecked the economy in 2008, the New Labour government asked global management consultancy company McKinsey to tell them how to cut NHS spending, because the government had spent £trillions bailing out the bankers.
McKinsey recommended making £20bn efficiency savings by 2015, although the New Labour government didn’t implement the planned cuts. It took the Coalition government to start the planned £20m the “efficiency” cuts in 2011. This is what drove our hospitals Trust into deficit in 2014.
At the same time Keogh, an NHS bigwig, started planning a new 3 tier urgent and emergency care system which is the blueprint for what is planned for Calderdale and Huddersfield:
- cutting A&E admissions by sending about half the patients who currently go to A&E to urgent care centres (like they want to replace HRI A&E with),
- sending patients with a range of life threatending conditions to a mid range Emergency Centre (which is what they’re proposeing for CRH) and
- sending some patients with life threatening conditions that need highly specialised care to a Specialist Emergency Centre eg Leeds General Infirmary.
The total number of A&Es is set to be hugely cut and at least a dozen have closed or been downgraded since 2011, with more in the pipeline.

The decision – or “preferred option” – to close Huddersfield A&E is the work of Monitor, the NHS market competition enforcer (kind of like Ofgem for the NHS), and Ernst and Young
Monitor imposed this global management consultancy company on the Trust, to produce a 5 year strategic plan telling the Trust what cuts to make over the next 5 years to cut its deficit.
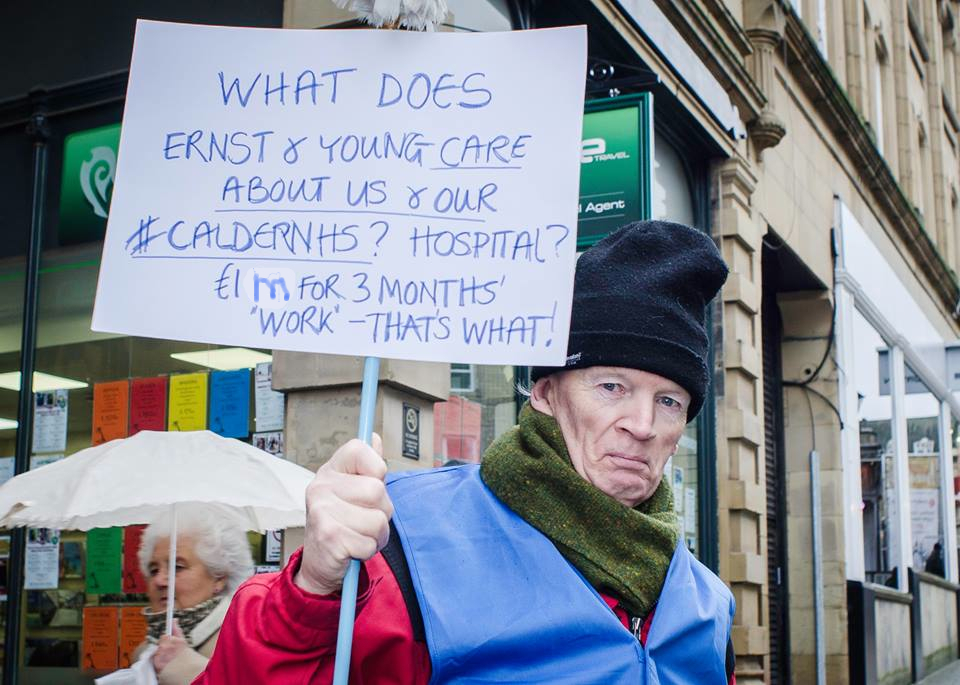
Dr Mike Galvin asks the £1m question
The Pre Consultation Business Case (p111) says that the preferred option was
“identified in CHFT’s 5 year Strategic Plan.”
After the Trust went into deficit in 2104 – along with 40% of the Foundation Trusts in England, all reeling under impossible government demands to make “efficiency savings” (ie cuts) – Monitor put the Trust in what are called enforcement measures. This basically means the Trust has to do what Monitor tells it.
At Monitor’s behest, Ernst and Young came in (at a fee of £511,600 for 3 months work) and told the Trust it had to protect the PFI banksters’ equity and profits above all else. Boom.
Sacrificing publicly owned hospitals to protect PFI bankers’ profits
This is happening everywhere there are PFI hospitals. The publicly owned hospitals are being sacrificed for the sake of the government’s bankster cronies and their profits.
This is part of a deliberate policy to run down the NHS by defunding it. It is designed to drive people to take out private health care insurance and to make it easier to sell off the NHS to private health care companies.
This was all laid down in a 1988 document by Tory MPs Oliver Letwin and John Redmond. The then Health Sec Ken Clarke suppressed it as electoral suicide.
30 years on it’s being implemented, with Oliver Letwin as Cabinet minister ie minister in charge of everything. It is the planned end game of the NHS after 30 years of drip drip drip stealth privatisation carried out by governments of all 3 main parties.
If you want to stop and reverse this, please support the cross-party NHS Reinstatement Bill and ask your MP to vote for it at its second reading in the House of Commons of 11th March.
It’s a good thing that we love uphill struggles

Here is a link to the downloadable Pre Consultation Business Case
Updated 31/1/2016 to correct the amount of the fee that CHFT paid Ernst and Young from £1m (the budgetted amount) to £511,600 (the amount spent).
Updated 11/2/2016 with the following links:
Here are links to some more Plain Speaker reports on the Pre Consultation Business Case proposals:
- “Care Closer to Home” – Patients Will Suffer
- Care Closer to Home – Too bad there’s little or no evidence it will work
- Impartial doctors can’t tell if unclear plan for Huddersfield hospital cuts & changes will provide required standard of care
- Wakefield and Dewsbury Hospitals Groaning Under “Clinical Model” Now Proposed for Calderdale & Kirkless
- A single “Emergency Care Centre” for both Calderdale and Kirklees – Not Safe, Not Fair
Plain Speaker reports on the proposed Consultation are here
Pingback: Please ask Councillors for public scrutiny of hospital cuts Consultation Document – Calderdale and Kirklees 999 Call for the NHS
Yorkshire Air Ambulance support our campaign #HandsoffHRI
Pingback: Scrutiny Committee must stop consultation on unfit Right Care hospital cuts scheme – Calderdale and Kirklees 999 Call for the NHS
Neighbouring North Kirklees CCG is the lead commissioner for the West Yorkshire Urgent Care Vanguard. They, alongside Greater Huddersfield CCG, Calderdale CCG the 3 Leeds CCGs, Airedale CCG, Harrogate CCG, Bradford CCG and 2 more, are all in line to have ‘Urgent’ provision commissioned on a regional level in the future. The move is towards the Devo Deception model flowering in Manchester and London.
Devo Deception – it’d be funny if it wasn’t awful.
And how does the Calderdale being chosen as a Vanguard site play into all this. It is obvious that it would be a major embarrassment to the government is the hospital was to fail. This whole reorganisation is designed to fit into this model.
The Calder Valley Multi-speciality Community Provider Vanguard fits in with the bit about moving services out of the hospitals, although it’s barely mentioned in the PCBC. I’ll be getting to that in an upcoming post. I agree this is all about imposing Simon Stevens’ “new care models” and “modern workforce” as laid out in his NHS England 5 Year Forward View.