
A crucial time for one of the main schemes to cut NHS services is now upon us.
From April 2016, NHS Foundation Trusts will be able to to stop providing certain NHS services, that are currently protected. This is due to changes to hospital licenses, brought in by the hospitals regulator and competition enforcer, Monitor.
At the Calderdale Clinical Commissioning Group meeting on 24th September 2015, Plain Speaker asked questions about how these licence changes are going to affect the range of services that Calderdale and Huddersfield hospitals provide.
Particularly: how this will affect Calderdale people’s access to comprehensive, universal healthcare that is free at the point of delivery and based on patients’ clinical needs. Given that it seems that services that are currently mandatory will fall away.
Calderdale Clinical Commissioning Group’s Accountable Officer gave some kind of reply at the meeting, and the CCG promised a written answer within 30 days. I’m still waiting.
I therefore asked the questions at the next meeting, on 8th October. Here are the questions and Matt Walsh’s reply, as recorded in the 8th October meeting Minutes:
Questions:
Could you please describe the Commissioner Requested Services the CCG plans to put in place after April 2016, and can you list the previously mandated services that will no longer be provided?
Do these changes represent a financially-driven rationing of the services that are currently available?
How will the CCG ensure the local population gets access to those services that are not Commissioner requested after April 2016?
Answer
Matt Walsh stated that
As previously mentioned in September, by the 1st April 2016 CCGs are required to review all commissioned services to establish which services theywished to continue in the event of a Foundation Trust going into special administration. In summary, this was a CCG contingency plan to protect access to those services they deem necessary. This was not, and should not be seen as the CCG’s strategic direction or commissioning intent.The nationally mandated process that had been followed, and the basis upon which the CCG would define a service as a Commissioner Requested Service, rested upon an analysis of other locally available NHS funded services and their use, through choice, by the CCG’s population.He said that this was an exercise specifically designed to ensure that the CCG’s population still had access to the full range of NHS funded services in the event of a local provider failing. If a service was not mandated as a Commissioner Requested Service, it indicated that there were other NHS providers offering those services already to the local population, and therefore the local provider was not a ‘sole provider’ of the service.
It was emphasized that this was not rationing and most assuredly was in the interests of the CCG’s local population to ensure that appropriate arrangements were in place to enable the population to get the NHS treatment they needed, should a local provider fail.
It was felt that the above response negated the two follow up questions.
It’s time for Calderdale and Kirklees Joint Health Scrutiny Committee to call in both Calderdale and Kirklees Clinical Commissioning Groups and use their review and scrutiny powers to find out which local services could potentially be stopped under the new April 2016 licences, and to object.
Time bomb set in 2012
This is a time bomb dropped by the Health & Social Care Act 2012. The Act re-designated mandatory hospital services as Commissioner Requested Services (CSRs).
This meant that some services that were once compulsory for Trusts to provide, became protected services that Commissioners had to request.
Now, from April 2016, Monitor is changing hospital licences so that these CSRs can lose their protection.
Monitor has told Clinical Commissioning Groups to review their Commissioners Requested Services. It has also given guidance to reduce their number, by the end of March 2016.
With profiteering management consultants Ernst and Young telling the Trust what services to cut to eliminate its deficit ( which is the result of years of government defunding the NHS), how will Calderdale CCG react to Monitor’s pressure to cut Commissioner Requested Services, come April 2016 when these hospital services no longer have to be provided?
Obviously the public need to know what they’re planning to do
What are these Commissioner Requested Services? We don’t even know what these at-risk services are.
So, these are my 24.9.15 questions to Calderdale Clinical Commissioning Group – which they’ve still not answered after nearly 60 days:
1) In 2013, what mandatory Calderdale and Huddersfield NHS Foundation Trust services were redesignated as Commissioner Requested Services, as a result of the HSCA 2012? Please give the full list.
2) In its review of Commissioner Requested Services, is Calderdale CCG going along with Monitor guidance to reduce the number of Commissioner Requested Services by end of March 2016? If so, what services are you taking off the list?
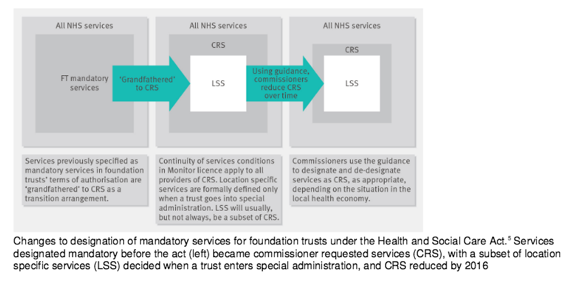
The context for my question 3 is this graphic, taken from a BMJ report, BMJ 2014;349:g5603 doi:10.1136/bmj.g5603. It shows Monitor’s guidance that locality-specific services (ie services that have to be provided if the Trust fails) should initially be a subset of Commissioner Requested Services; but that over time these two services will converge, as Commissioner Requested Services reduce.
3) From Calderdale Clinical Commissioning Group’s Right Care Right Place Right Time report (which says that Commissioner Requested Services are services which the commissioner has decided must stay in the locality if the Trust fails), it seems that the CCG has already converged CRS with locality-specific services that have to be provided if the Trust fails. Why has the CCG taken this step?
4) Please explain the effects of all this on Calderdale people’s access to comprehensive, universal healthcare that is free at the point of need – given that it seems that services that are currently mandatory will fall away, so that NHS-funded care in both hospital and community services provided by the Trust will eventually be limited to the locality-specific services that have to be provided in the event of Trust failure.
This further undermines the principle of the NHS as a comprehensive universal health service, that the HSCA 2012 eroded by removing the Secretary of State’s duty to provide such a service.
Updated 5 October 2017 to include Matt Walsh’s minuted response to the questions I asked again at the 8th October 2015 meeting.